At its core, a medical record summary is a straightforward, chronological overview of a patient's medical history. It's the art and science of taking what can be thousands of pages of dense, complex files and distilling them into a clear, easy-to-follow narrative.
Think of it as the roadmap your legal team needs to quickly get a handle on the facts of a case, without getting hopelessly bogged down in the raw medical data.
Why a Medical Record Summary Matters in Legal Cases
Ever tried to build a legal argument from a mountain of disorganized medical files? It’s a nightmare. You’re dealing with reports from a dozen different doctors, hastily scribbled nurses' notes, and duplicate lab results that create a chaotic, nearly impossible puzzle.
This is exactly where the medical record summary proves its worth. It acts as your most powerful strategic tool, transforming that overwhelming mess of data into a streamlined, chronological story.
It’s less of a document and more of a high-powered lens. It brings the critical details of a case into sharp focus while filtering out all the irrelevant noise. For any personal injury attorney, that kind of clarity isn't just helpful—it's essential.
The Foundation of Legal Strategy
A well-crafted summary doesn’t just list events; it lays the very foundation for your entire legal strategy. It empowers legal professionals to:
Grasp Case Facts Quickly: Forget spending dozens of hours piecing together a timeline from scratch. A good summary gives you the core narrative in minutes.
Identify Critical Events: The summary immediately highlights the key moments—the initial injury, specific diagnoses, and crucial treatment decisions that define the case.
Strengthen Negotiations: When you can present a clear, evidence-based account of your client's medical journey, you walk into settlement discussions with a much more compelling argument.
Pinpoint Inconsistencies: It’s also brilliant at revealing gaps in treatment or conflicting reports that can become pivotal points during litigation.
A medical record summary isn't just about condensing information; it’s about creating legal clarity. It converts a complex medical history into a persuasive narrative that can make or break a case.
Ultimately, the medical record summary is the bridge between raw medical facts and a winning legal argument. It provides the structure you absolutely need to establish causation, document the full scope of damages, and confidently prepare for depositions and trials. Without one, you're just navigating the complexities of a case without a map.
Anatomy of a Powerful Summary
What’s the real difference between a summary that sits in a file and one that actually wins a case? It all comes down to how it's built. A truly effective medical record summary isn’t just a list of facts; it’s a carefully constructed narrative where every component serves a strategic purpose.
Think of it like an engine. You can have all the parts, but if they aren't assembled in the right order and working in harmony, you've just got a pile of metal. Miss one small piece, and the whole thing can seize up.
Core Informational Pillars
Every solid summary is built on a foundation of essential data points from each medical encounter. These are the non-negotiable facts that form the skeleton of your client's medical journey.
Dates of Service: The exact start and end dates for every visit, procedure, or hospital stay. This is the bedrock of your timeline.
Healthcare Providers and Facilities: Who provided the care and where? You need a clear list of every doctor, specialist, hospital, and clinic involved to map out the network of treatment.
Diagnoses and Conditions: A straightforward list of every official diagnosis, complete with ICD codes whenever possible. This defines the core medical problems.
Treatments and Procedures: What was actually done? This includes everything from major surgeries and physical therapy to prescribed medications and MRI scans.
Medication History: A running log of every prescription—drug name, dosage, frequency, and how long it was taken.
This information is your raw material. Thankfully, the widespread adoption of Electronic Health Records (EHRs) has made gathering this data a bit more predictable. In the U.S. alone, over 95% of hospitals have moved to EHR systems, a huge leap from just 12% back in 2009. This digital shift is credited with boosting healthcare efficiency by an estimated 30% worldwide, which means legal teams often have more structured data to start with. You can explore more about EHR adoption trends and what it means for data access.
The infographic below shows how messy, raw medical files get refined into a sharp legal instrument.
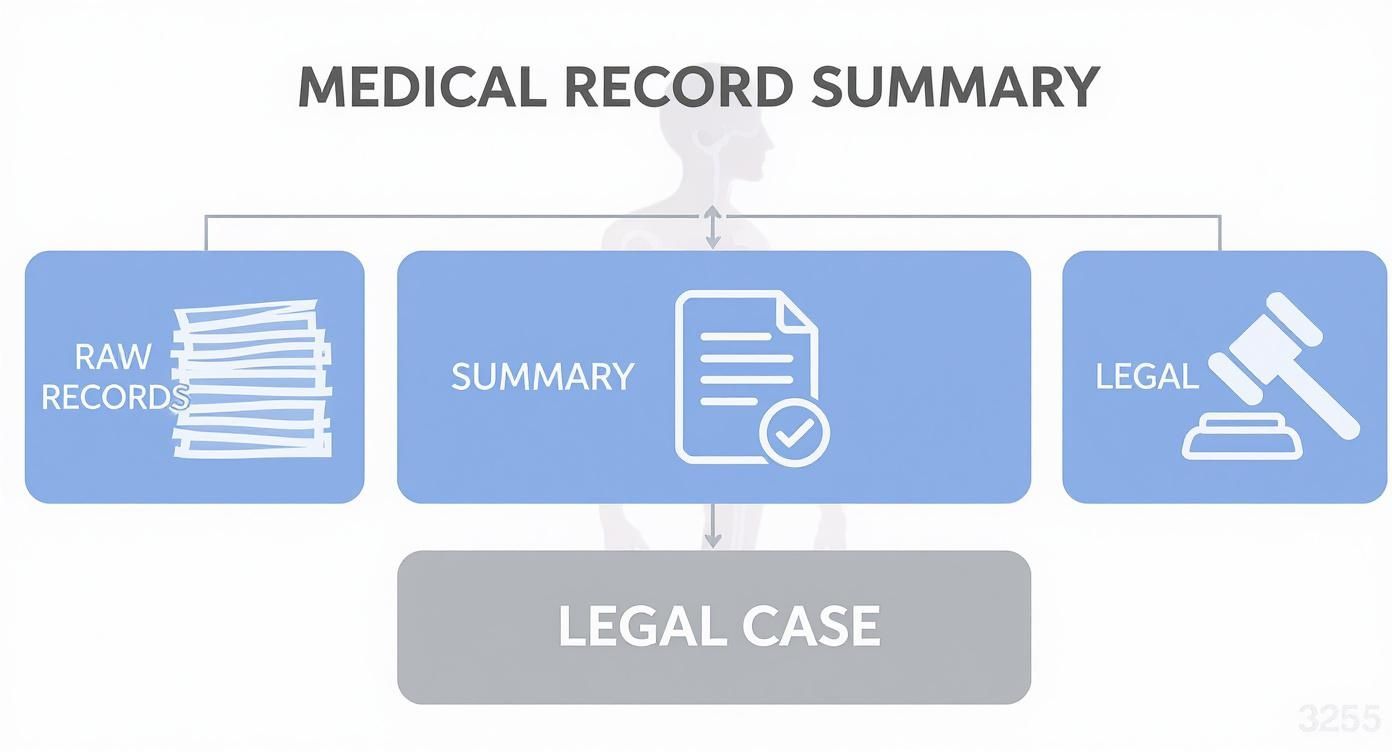
As you can see, the summary is the critical bridge. It takes a mountain of disorganized data and translates it into a clear, usable format that’s ready for legal battle.
Uncovering the Strategic Narrative
A powerful summary does more than just list what happened. It connects the dots to reveal the story hiding in the data. This is where a simple chronology of events transforms into a strategic weapon for your case.
A great summary doesn’t just report what happened; it highlights the significance of what happened—and just as importantly, what didn't happen.
This means you have to be an active investigator, looking for and flagging the elements that truly shape the narrative:
Chronological Flow: Does the patient’s journey make sense? The summary must lay out a clear timeline from injury to diagnosis, treatment, and the recovery process.
Treatment Gaps: Were there long, unexplained breaks in care? Spotting these gaps early allows you to get ahead of the inevitable defense argument that your client failed to mitigate their damages.
Conflicting Information: Do notes from the primary care physician contradict what the specialist wrote? Highlighting these inconsistencies is crucial for avoiding ugly surprises in depositions or discovery.
By digging into these components, you elevate a basic medical record summary from a simple reference document to a dynamic tool. It becomes a tool that builds your argument, anticipates the other side’s moves, and ultimately strengthens your entire case.
Building Your Case with a Strategic Summary
A well-crafted medical record summary is far more than just a list of facts; it’s the narrative that frames your entire legal strategy. You shouldn't think of it as a passive document. It’s an offensive tool, especially in a personal injury case. This is how you transform a messy, scattered medical history into a clear story that proves cause, effect, and consequence.
This is where the summary stops being about organization and starts being about argumentation. By laying out a clear, chronological timeline of events, you draw a direct line from the incident to the injuries and all the treatments that followed. This story becomes the backbone of your case, supporting everything from the initial demand letter to settlement talks and even trial preparation.
From Causation to Compensation
The real power of a medical record summary is its ability to build a persuasive argument, piece by piece. Take a car accident case, for instance. The summary doesn't just state the client has a back injury. It shows the client had no history of back pain before the crash, that they went to the emergency room immediately after, and that they consistently followed up with orthopedic specialists.
This chronological proof is crucial for hitting several key legal goals:
Establishing Causation: The timeline connects the defendant's negligence directly to the plaintiff's injuries, making it much harder to dispute the link.
Documenting Full Extent of Injuries: It captures the complete picture of the harm—physical, emotional, and psychological—by detailing every diagnosis, treatment, and therapy session.
Calculating Damages: By itemizing all the medical bills, prescriptions, and recommended future care, the summary gives you the hard data needed to accurately calculate economic damages.
Countering Defenses and Preparing for Trial
A smart summary also plays defense by helping you get ahead of the other side's arguments. We've all seen it—insurance adjusters and defense attorneys love to claim injuries were pre-existing or that the plaintiff didn't follow their doctor's orders.
The chronological flow of a medical record summary is your best weapon against claims of pre-existing conditions. It creates an undeniable record of the client's health status before the incident and the clear change afterward.
A detailed timeline shuts these arguments down. It highlights continuous care, proving the client was proactive in their recovery. It also flags any gaps in treatment, which allows you to prepare an explanation instead of being blindsided during a deposition.
Ultimately, this level of detailed preparation gives you a powerful, evidence-based story for every stage of litigation. For firms wanting to build these strategic narratives faster, understanding how AI can automate medical records review is a game-changer, turning days of manual work into just minutes of focused analysis.
Best Practices for Accuracy and Compliance

Putting together a medical record summary that holds up in court requires more than just careful work—it demands a strict, methodical approach. The end goal is to create a document that accurately mirrors the original records and can withstand the intense scrutiny it will inevitably face from opposing counsel and insurance adjusters.
Think of your role as a neutral narrator, not a storyteller. Your job is to lay out the facts exactly as they appear in the records. Forget adding your own spin, interpretations, or any emotional language. A summary's true power is its objectivity; the second it feels biased, its credibility is gone.
This means you must stick to the verifiable information found within the files. Don't make assumptions about what caused an injury or jump to conclusions that a healthcare provider hasn't explicitly stated in their notes.
Maintaining Objectivity and Precision
To make sure your summary is both accurate and impartial, there are a few core principles to live by. These guidelines are essential for maintaining the document’s integrity and making it a reliable tool in any legal setting.
Quote Verbatim: When you're documenting a patient's complaints or a doctor's diagnosis, use direct quotes from the record. This eliminates any risk of misinterpretation.
Define Jargon: If you have to include complex medical terms or abbreviations, make sure you define them clearly the first time they appear. An undefined term just creates confusion and can weaken your position.
Verify and Cross-Reference: Always compare information across different provider notes. If a specialist's diagnosis conflicts with what the primary care physician wrote, that discrepancy must be noted in the summary.
A truly effective medical record summary is an exercise in disciplined restraint. It conveys the full story by sticking strictly to the documented facts, letting the evidence speak for itself without added commentary.
One of the biggest mistakes people make is overlooking conflicting details. Pointing out these inconsistencies doesn't hurt your case—it actually makes it stronger by demonstrating thoroughness and preparing your legal team for the challenges ahead.
Common Pitfalls vs Best Practices in Summary Creation
It's easy to fall into bad habits when summarizing dense medical records. The table below contrasts some of the most frequent mistakes with the best practices that ensure your summary is accurate, defensible, and professional.
| Common Pitfall | Best Practice Solution |
|---|---|
| Using subjective language (e.g., "excruciating pain") | Quote directly from the record (e.g., Patient reports "10/10 sharp pain"). |
| Ignoring conflicting information | Document all discrepancies between provider notes to present a full, transparent picture. |
| Making assumptions about causation | Only state what is explicitly written by a medical professional. Avoid connecting events unless the record does. |
| Leaving medical jargon undefined | Define all abbreviations and complex terms on their first use (e.g., "ROM - Range of Motion"). |
| Summarizing out of chronological order | Maintain a strict timeline to accurately show the progression of care and the sequence of events. |
By consciously avoiding these common errors and sticking to best practices, you ensure the final document is a tool that helps, rather than harms, your case.
Upholding HIPAA and Data Security
Beyond just getting the facts right, compliance with the Health Insurance Portability and Accountability Act (HIPAA) is absolutely non-negotiable. Mishandling Protected Health Information (PHI) can lead to severe legal and financial penalties, with civil fines that can climb past $2 million per violation.
Every single step of the summarization process must prioritize data security. This means controlling who can access the records, tracking every interaction with the files, and making sure any digital platform you use is secure.
For any firm dealing with sensitive client data, understanding the technical safeguards is crucial. You can learn more about the importance of enterprise-grade security protocols when handling PHI. By following these best practices, you'll produce a medical record summary that is not just accurate but also ethically and legally sound—ready to serve as a reliable foundation for your case.
AI Is the New Standard for Medical Summaries
The days of paralegals spending weeks manually digging through thousands of pages of medical records are fading fast. That painstaking process—organizing, cross-referencing, and summarizing dense files—is being completely reshaped by artificial intelligence.
Think of it this way: AI-powered platforms act like a super-powered assistant, one that can read an entire medical history in minutes, not days. This technology doesn't just scan words; it understands context, pinpoints critical events, and weaves a coherent story from scattered files.
This shift turns the creation of a medical record summary from a draining administrative chore into a swift, strategic part of your workflow. For law firms, the benefits are immediate and undeniable.
More Speed, Better Accuracy
The most obvious win with AI is the incredible time savings. A task that once took a skilled paralegal over ten hours to complete for a single case can now be done in just a few minutes. This frees up your legal team to focus on what they do best: building case strategy, prepping for depositions, and negotiating settlements.
But it’s not just about speed. AI brings a whole new level of precision to the table.
Fewer Human Errors: An AI system doesn't get tired or miss a crucial detail buried on page 800 of a record. It consistently flags dates, diagnoses, and treatments, cutting down on the risk of costly mistakes.
Deeper Data Extraction: These tools pull information from both structured fields and unstructured notes, finding connections between a doctor’s scribbled comment and a lab result that a human reviewer could easily overlook.
Unbiased Analysis: AI presents the facts exactly as they appear in the records, free from the unintentional bias that can sometimes color a manual summary.
This evolution is happening right as digital health information is exploding. The global Electronic Medical Records (EMR) market was valued at USD 33.41 billion in 2025 and is projected to hit USD 49.62 billion by 2032, largely because AI is making this data more useful. You can read more about the growth of the EMR market and its wider impact.
The process is surprisingly simple. As you can see in this example from Ares Legal's platform, users just upload their files and let the technology do the work.
This clean interface gets rid of all the manual sorting and replaces it with an efficient drag-and-drop system.
Rock-Solid Security and Compliance
Of course, when you're handling sensitive Protected Health Information (PHI), security is non-negotiable. The top AI platforms in legal tech are built with this in mind from the ground up. They use enterprise-grade security and are designed for full HIPAA compliance, so you can be confident that all client data is locked down.
By automating the summarization process, AI not only accelerates case preparation but also introduces a more consistent, accurate, and secure method for handling critical medical evidence.
This powerful combination of speed, accuracy, and security is what makes AI an essential tool for any modern personal injury firm. It gives your team the ability to manage a larger caseload without ever sacrificing the quality and detail needed to build a winning argument. To learn more about how firms are putting these tools into practice, check out our guide on innovations in legal technology. The future of the medical record summary isn't just faster—it's smarter.
Frequently Asked Questions
It's natural to have questions when you're wading through the details of creating and using a medical record summary. Let's tackle some of the most common ones that come up for legal professionals, clearing up the key differences, time commitments, and the role of new technology.
How Is a Summary Different from Raw Medical Records?
Think of it this way: raw medical records are like the complete, unedited director's cut of a film. Every single scene, outtake, and note is in there, but it's overwhelming and you have to dig through hours of footage to find the plot.
A medical record summary is the final, edited movie. It's the tight, chronological narrative that tells the story. It pulls out only the crucial plot points—the injuries, diagnoses, and treatments—and presents them in a way that’s easy for anyone to follow. The raw records are the evidence; the summary is what makes that evidence compelling and useful in a legal setting.
How Long Does It Take to Create a Summary Manually?
This is the million-dollar question, and the answer really depends on the case. For a straightforward personal injury case with a few hundred pages of records, a sharp paralegal might knock it out in 5-10 hours.
But for a complex case with years of medical history, multiple specialists, and thousands of pages? You’re easily looking at 20-40 hours, maybe even more.
That huge time commitment is exactly why AI-powered tools are changing the game. They can turn a task that takes days or even a week into a matter of minutes. This frees up your team to focus on building a winning strategy instead of getting buried in paperwork.
Is an AI-Generated Summary as Reliable as a Human-Made One?
Yes, and in many ways, it can actually be more reliable. A human paralegal brings incredible insight to the table, but they're still human. Fatigue, distractions, and simple oversight can lead to missed details or unintentional errors, especially after hours of staring at dense medical charts.
AI, on the other hand, is built for precision. It doesn't get tired and it doesn't skim. It meticulously scans every page, ensuring no critical date, diagnosis, or treatment gets missed. This provides an incredibly accurate and objective foundation that a legal professional can then review and layer with their own strategic insights.
The industry is taking notice. The global market for medical records retrieval was valued at USD 1.1 billion in 2024 and is projected to skyrocket to USD 2.8 billion by 2034. This growth is overwhelmingly driven by AI tools that deliver speed and security. You can read more about the expansion of the medical records retrieval market to see just how big this shift is.
Ready to stop drowning in manual reviews and start building stronger cases faster? The Ares Legal, LLC platform handles your medical record summaries and demand letter drafting in minutes, giving your firm a real competitive edge. Start your free trial today and see the difference.